Femoroacetabular Impingement (FAI)
(AKA: Femoral Acetabular Impingement, Femoro-Acetabular Impingement)
![]()
Follow on X @HipFAI
What is it?
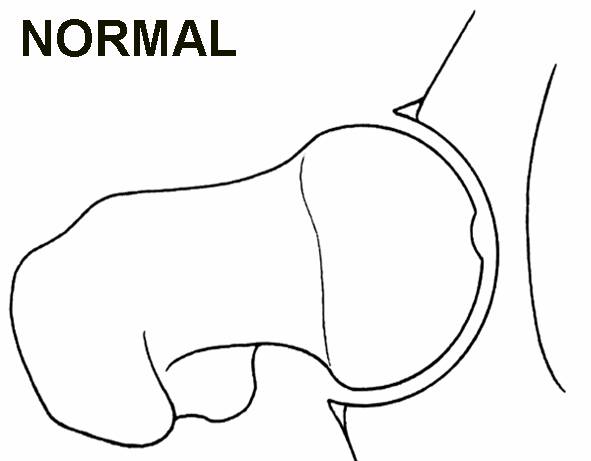
Femoroacetabular impingement or FAI is a condition of too much friction in the hip joint. Basically, the ball (femoral head) and socket (acetabulum) rub abnormally creating damage to the hip joint. The damage can occur to the articular cartilage (smooth white surface of the ball or socket) or the labral cartilage (soft tissue bumper of the socket).
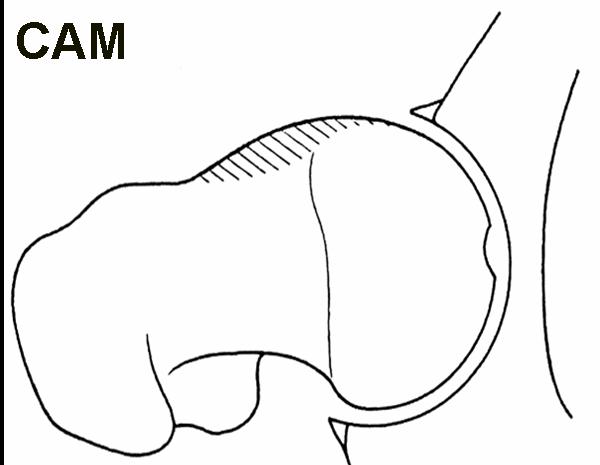
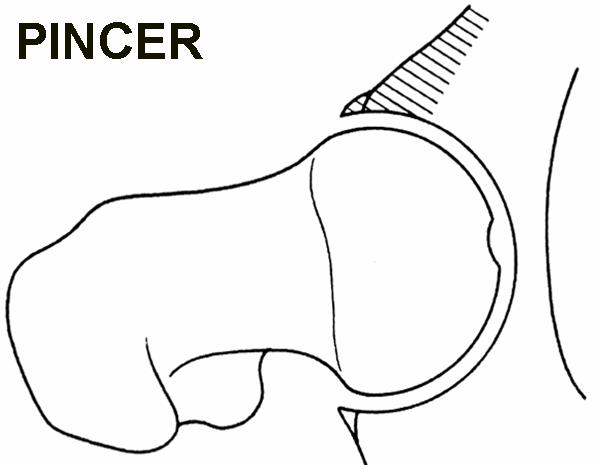
FAI generally occurs as two forms: Cam and Pincer. The Cam form (Cam comes from the Dutch word meaning “cog”) describes the femoral head and neck relationship as aspherical or not perfectly round. This loss of roundness contributes to abnormal contact between the head and socket. The Pincer form (Pincer comes from the French word meaning “to pinch”) describes the situation where the socket or acetabulum has too much coverage of the ball or femoral head. This over-coverage typically exists along the front-top rim of the socket (acetabulum) and results in the labral cartilage being “pinched” between the rim of the socket and the anterior femoral head-neck junction. The Pincer form of the impingement is typically secondary to “retroversion”, a turning back of the socket, “profunda”, a socket that is too deep, or "protrusio", a situation where the femoral head extends into the pelvis. Most of the time, the Cam and Pincer forms exist together- i.e., "mixed impingement"..
FAI is associated with cartilage damage, labral tears, early hip arthritis, hyperlaxity, sports hernias, subspinous AIIS impingement, ischiofemoral impingement, and low back pain.
FAI is common in high level athletes, but also occurs in active individuals.
 |
 |
 |
 |
The diagnosis can be straightforward or a diagnosis of exclusion. Most patients can be diagnosed with a good history, physical exam, and plain x-ray films. A patient’s history will generally involve complaints of hip pain (front, side, or back) and loss of hip motion. The physical exam will generally confirm the patient’s history and eliminate other causes of hip pain. The plain x-ray films are used to determine the shape of the ball and socket as well as assess the amount of joint space in the hip. Less joint space is generally associated with more arthritis.
Often an MRI of the hip is used to confirm a labral tear or damage to the joint surface. The MRI is most helpful in eliminating certain causes of non FAI hip pain including avascular necrosis (dead bone) and tumors. A normal MRI does not preclude cartilage injury, labral tears, or FAI.
What studies should my doctor order?
In most cases, a Supine AP Pelvis view and a Hip Cross Table Lateral View are sufficient. The Pelvis view should be taken so that the coccyx projects 1.5 cm above the symphysis pubis. The Lateral view should be made with the lower extremity internally rotated 15 degrees. As the x-ray films are the most important part of the diagnosis, they should be no older than three to six months and of good quality.
An MRI should be ordered as a left or right hip study with consideration for intraarticular gadolinium (contrast dye in the joint) and a pain test. The pain test typically involves placing a local anesthetic inside the hip joint with the contrast dye. The pain test may help assess whether the pain is coming from inside the hip joint.
Can back pain be a sign of FAI?
Yes. While the cause is not well understood, patients with FAI often complain of low back pain. This pain is often localized to the SI (sacroiliac joint on back of pelvis), the buttock, or greater trochanter (side of hip). FAI associated pain typically does not go beyond the level of the knee.
What other diagnoses might be confused with FAI?
Hip Dysplasia (Adult Form)
Lumbar Spine Pain (Low Back Pain)
Lumbar Radiculopathy (Low Back Pinched Nerve, Low Back Facet Disease)
Sacroiliitis (SI Pain/Dysfunction, back of pelvis)
Trochanteric Bursitis (Outside/Lateral Hip Pain)
Piriformis Syndrome (Back of Hip Pain)
Psychosomatic Pain Disorder (Stress Related Illness)
Iliopsoas Tendinitis/Tendonitis/Tendinosis (Hip Flexor Inflammation)
Ischiofemoral Impingement (IFI)
Subspinous (AIIS) Impingement
Groin Pull (Adductor Strain)
Sports Hernia (Core Muscle Injury (CMI), abdominal muscle strain)
Iliac Apophysitis (Front of Pelvis Pain)
Quadriceps Hernia/Strain (Thigh Muscle Pull)
Endometriosis
Deep Gluteal Syndrome (DGS)
Hamstring Tendinitis/Tendinosis
Chronic Pain Syndromes
With what activities is FAI associated?
Some common activities
Ice Hockey
Horseback Riding
Yoga
Football (American)
Soccer
Ballet/Dance/Acrobatics
Golf
Tennis
Baseball
Lacrosse
Field Hockey
Rugby
Bike Riding/Cycling
Martial Arts and Mixed Martial Arts
Deep squatting activities such as power lifting
Surfing
Rowing Sports (Kayaking, Sculling/Rowing)
Car riding, Flying in an airplane (deep seated position, bucket seat position)
Why does it occur?
No one knows if FAI is a condition that begins at birth (congenital and genetic association) or develops during periods of growth (acquired). It is likely a combination of one’s genetics and environment.
How did I get it?
Some experts believe that significant athletic activity before skeletal maturity increases the risk of FAI, but no one truly knows. Significant contact sports (i.e., football) and male gender are associated with Cam impingement. Pincer type impingement may be more common in women.
Do I have arthritis if I have FAI?
Both plain film x-rays and MRI scans are an incomplete view of the cartilage inside the hip joint. It is possible and common to have good joint space on plain x-ray films and no signs of arthritis on MRI and still have significant loss of cartilage within the hip.
Do I have FAI if my hip MRI was read as “Normal”?
At times, an MRI will be read as “Normal” but the clinical history, physical exam, and plain x-ray films indicate FAI. In this situation, further investigation with an arthroscopic surgery may be needed.
My doctor told me that I have hip dysplasia, is this FAI?
Hip dysplasia (adult form) and FAI are two separate theories to account for degenerative hip disease and hip pain. Hip dysplasia is basically a hip condition where, most commonly, the socket (acetabular) coverage of the hip ball (femoral head) is insufficient or "too shallow". Ultimately, the contact forces within a dysplastic hip joint are more concentrated than in a non-dysplastic hip joint with sufficient socket (acetabular) coverage of the hip ball (femoral head). Hip dysplasia is associated with tearing of the labral and articular cartilages. In some circumstances, adult hip dysplasia may be present with FAI. Hip dysplasia may be treated with a type of surgery called a "PAO- periacetabular osteotomy".
What is an Alpha angle?
The Alpha angle refers to a measurement taken of the hip ball (femoral head and neck junction) to determine how much Cam impingement exists. The Alpha angle measurement can be taken on plain film xray, CT scans, or MRI scans. The larger the Alpha angle, the larger the Cam impingement lesion. By convention, an Alpha angle greater than 50 to 55 degrees may be considered indicative of CAM morphology. The Alpha angle is most accurate when obtained from a special MRI scan that controls for hip rotation. An alpha angle is not essential to the diagnosis of FAI.
My doctor recommended a CT scan of my hip to evaluate for FAI, should I follow this recommendation?
A CT or CAT scan is often helpful in understanding the anatomy of the bones of the hip joint, but not essential to the diagnosis of FAI. One should balance the large amount of radiation to the pelvis/reproductive region with the amount of information obtained. This concern of additional radiation is especially important when 3-D CT scans are performed.
My doctor recommended an MRI with IV contrast [dGEMERIC MRI study] instead of contrast in the hip joint (MRI Arthrogram) to evaluate for FAI, should I follow this recommendation?
An MRI scan with IV contrast [dGEMERIC] is an experimental study used to understand the condition of the hip joint cartilage. It is not essential to the diagnosis of FAI.
My diagnosis was made after many years of hip pain, is that common?
Many physicians have heard of a hip labral tear but have not heard of FAI.
I’ve been treated for a labral tear with a hip arthroscopy. Could I have FAI, too?
Hip labral tears are associated with FAI. If you have had your labral tear treated and are still having pain, you may have unrecognized FAI and additional cartilage degeneration/tearing. This FAI may accelerate the loss of hip cartilage leading to further degeneration. Labral debridement is not the same as labral repair.
Can my other hip be involved as well?
Yes, it is possible for both hips to have FAI.
I don’t have any pain, what should I do?
Some patients with FAI complain of stiffness and loss of hip range of motion without any significant pain. Progressive loss of motion in the hip can be associated with ongoing FAI. Speak to your physician about your options.
My doctor says that FAI doesn’t exist, why?
Currently, three different opinions exist regarding hip pain and hip problems. The first is that all hip problems are generally mild and should be managed with nonoperative choices such as injections, therapy or rest. If there is severe hip arthritis, a total hip replacement is considered. The second is that hip problems often involve labral tears and that these tears can be treated by cutting out the torn tissue– usually with an arthroscopy. The third is that hip problems often involve labral tears and that these tears are often secondary to abnormal hip biomechanics such as the labrum getting caught by friction between the bone of the ball (femoral head) and the bone of the socket (acetabulum)- the condition of FAI. This third approach often leads to surgical treatment of the bone and soft tissue problems of FAI.
What type of doctor can treat it?
If one has a diagnosis of FAI or suspects FAI, one should be evaluated by an orthopaedic hip preservation specialist. Your physician should have experience with either open surgical hip dislocation or hip arthroscopy.
What are my treatment options?
Nonoperative management of FAI is possible; however, it involves a change in lifestyle from active to less active and a commitment to maintaining hip strength. Nonoperative management will not change the underlying abnormal hip biomechanics of FAI and may contribute to further hip degeneration..
Operative management of FAI can be addressed via hip arthroscopy or open surgery. In hip arthroscopy, the hip is distracted and an arthroscope is used to make an assessment of the hip joint and treat damage that is found through two to four 1 cm incisions. Often, all of the components of FAI such as the labral tear, damaged cartilage, and friction between the ball and socket can be treated through the arthroscope. Repair of a torn labrum as well as stimulating new cartilage growth (microfracture) are often possible with the arthroscopic approach. A hip arthroscopy involving labral debridement (no repair) and no bony decompression usually takes less than one hour. A hip arthroscopy involving labral/cartilage repair and FAI decompression may take between two and four hours, depending on the amount of work performed. Care must be taken to avoid damage to the hip's blood supply (the retinacular vessels) during the osteoplasty procedure.
The open surgical hip dislocation involves an incision (approximately 6 to 10 inches), an osteotomy or bone cutting of the upper thigh bone, and dislocation of the ball from the socket exposing all parts of the joint. This exposure allows treatment of labral tears and abnormal contact between the ball and socket while protecting the blood supply to the hip. The open approach can typically be done in a few hours. The open approach is not generally recommended in older patients, in patients with significant hip degeneration, or in patients with significant athletic/activity demands..
Recovery time from most arthroscopic FAI surgical procedures is about 3 to 4 months to full, unrestricted activity. Your postoperative activity level will depend on your surgeon’s recommendation, the type of surgery performed, and the condition of the hip joint at the time of surgery. Revision FAI surgery may involve a significantly longer recovery.
What are the central, peripheral, and lateral compartments of the hip?
During a hip arthroscopy, the surgeon should visualize two compartments or spaces of the hip joint. The first space is the central compartment. The central compartment is composed of the surfaces of the ball (femoral head) and the socket (acetabulum) as well as the soft tissues (i.e., labrum). Procedures performed within the central compartment include treatment of the cartilage and labrum. The peripheral compartment is the remainder of the hip joint and refers to the area along the junction of the femoral head (ball) and femoral neck. Procedures performed within the peripheral compartment include treatment of bone spurs and the joint capsule. Both the central and peripheral compartments are within the hip joint capsule making them accessible with the arthroscope. The lateral or peritrochanteric compartment lies outside of the hip joint. The surgeon may enter the lateral compartment with the arthroscope to evaluate and treat disorders such as hip muscle/tendon tears, snapping hips, piriformis syndrome, and hip inflammation (trochanteric bursitis).
What are the main risks of FAI treatment?
Complications from FAI hip surgery are uncommon but include the following:
DVT (blood clot)
Infection
Hip Instability & Dislocation
Femoral neck fracture
AVN of the femoral head (dead bone)
Heterotopic ossification (abnormal bone formation in soft tissues)
Nerve injury (Sciatic, LFCN, Pudendal, Peroneal)
Nonunion (open surgical dislocation only)
Scarring/Adhesions
How long can I wait before seeking treatment?
Typically, FAI that produces symptoms should be evaluated for surgical treatment. A delay in FAI treatment may compromise the cartilage of the hip.
Can I be treated with an injection of medicine or good physical therapy?
Generally, FAI is a chronic condition that does not typically respond to hip injections or physical therapy over the long term. That being said, a good physical therapy program focusing on core strengthening instead of hip stretching may be beneficial. In fact, the stretching associated with yoga may make the symptoms worse.
Can I just wait a few years and have a total hip replacement?
Yes. The postoperative rehabilitation of a total hip replacement (total hip arthroplasty) is significantly less than an FAI procedure; however, the lifespan of the replacement hip is shorter in younger patients. The same is true for a hip resurfacing type of procedure such as the Birmingham Hip Resurfacing Arthroplasty. Both the resurfacing arthroplasty and the total hip arthroplasty involve amputation of the diseased joint surfaces and replacement with man-made materials (i.e., metal, plastic, ceramic) which are subject to wear. The wear results in joint debris which may shorten the life of the replacement. Finally, the use of metal-on-metal hip bearings is controversial in women of childbearing age and in patients with metal sensitivities.
DISCLAIMER: This site is not intended to diagnose, treat, cure, or manage an illness. Please consult your physician.
Copyright Protected © 2006-2024 Ortho Enterprises, LLC
All Rights Reserved
Share With Others! Follow on X @HipFAI
![]()